Pātiki and Waharua Kōpito patterns
On this page
Key information
|
Mode of transmission |
Zoster is a reactivation of the varicella-zoster virus in someone who has previously had varicella disease (most often as chickenpox). Direct contact with zoster vesicles has a low risk of causing varicella in non-immune individuals – can be prevented by covering the rash. There is potential for aerosol transmission from some immunocompromised cases with viraemia. |
|---|---|
|
Period of communicability |
Until lesions have crusted. |
|
Incidence and burden of disease |
Increasing incidence with age; lifetime risk about 1 in 3. For those aged over 85 years, the risk is 1 in 2. Complications include post-herpetic neuralgia and herpes zoster ophthalmicus. |
|
Funded vaccine |
Recombinant zoster vaccine – rZV; Shingrix |
|
Dose, presentation, route |
|
|
Funded vaccine indications and recommended schedule |
Two doses of rZV given 2 to 6 months apart.
|
|
Recommended, not funded |
|
|
Vaccine efficacy/ effectiveness |
rZV showed efficacy against both zoster and post herpetic neuralgia of over 90 percent in participants aged over 50 years and over 70 years, including those with comorbidities, maintained at 84 percent for at least 7 years and at 70 percent for up to 10 years. |
|
Contraindications and precautions |
For contraindications and precautions see section 25.6.1. Use in pregnancy is limited and not routinely recommended. |
|
Potential responses to vaccine |
Injection-site pain, myalgia, headache and fatigue are the most common responses. |
25.1. Virology
Varicella-zoster virus (VZV) is a DNA virus from the herpesvirus family. The virus is usually acquired in childhood and primary infection with VZV causes varicella disease (chickenpox). Herpes zoster (zoster), or ‘shingles’, is a clinical syndrome caused reactivation of latent VZV, which resides in the dorsal root or trigeminal nerve ganglia after primary infection. VZV is usually acquired in childhood, but it is often many decades before the virus reactivates, at times when cellular immunity is compromised and is unable to maintain suppression of the virus.
25.2. Clinical features
Herpes zoster (shingles) occurs when the cell-mediated immune response is impaired and unable to maintain suppression of latent varicella-zoster virus reactivation (see chapter 24). Zoster occurs only by loss of suppression and reactivation of the patient’s own virus – which is often acquired in childhood; it is not acquired from other patients with zoster or varicella.[1]
VZV, present at low levels in lesions of zoster rash, is transmissible via direct contact with fluid in the rash vesicles to VZV-naïve or other susceptible individuals (causing chickenpox). Episodes of zoster in older individuals provide a constant mechanism for reintroducing the virus, causing varicella in non-immune individuals who are in close contact, who then spread the virus to other susceptible individuals. Covering the rash can reduce this risk of transmission.
Zoster presents clinically as a unilateral vesicular rash, which in most cases is in a dermatomal distribution. The dermatomal distribution of the rash is the key diagnostic feature. In 70–80 percent of zoster cases in older adults, prodromal pain and/or itching occurs three to four days before the appearance of the rash.[2] In the majority of patients, zoster is an acute and self-limiting disease, with the rash lasting 10–15 days. However, complications can occur, especially with increasing age.
Although most zoster cases occur in adults aged 40 years or older, it may be seen less commonly in infants and children. In those aged under 2 years may reflect in utero chickenpox, with the greatest risk arising following exposure between 25 and 36 weeks’ gestation, and reactivation in early life. Infants who get varicella at a young age have a higher change of having zoster before the age 20 years.
A common complication of zoster is post-herpetic neuralgia (PHN), a chronic, often debilitating pain condition that can last several months or even years. A systematic review of the incidence and complications of zoster found that the risk of developing post-herpetic neuralgia ranges between 5 percent and about 30 percent (depending on the type of study design, age distribution of the study populations and definition).[3] The risk rises with age, and it is uncommon in healthy children and young people.
Herpes zoster ophthalmicus (HZO) is another complication of zoster, which occurs when VZV reactivation affects the ophthalmic branch of the trigeminal nerve. HZO can occur with or without eye involvement, and can result in prolonged or permanent pain, facial scarring and loss of vision. About 10 percent of zoster patients develop HZO, if that dermatome is affected, and the risk is similar across all age groups.[3]
The incidence of zoster is highest in immunocompromised individuals,[4, 5] including:
- following HSCT
- solid organ transplants[6]
- haematological malignancy[7]
- immunomodulatory treatments and immune-mediated inflammatory diseases including treatments for
- rheumatoid arthritis[8]
- systemic lupus erythematosus
- inflammatory bowel disease
- cancer
- those living with HIV infection.
Up to 10 percent of children treated for a malignant neoplasm may develop zoster. In immunocompromised patients, extensive viraemia in the absence of a vigorous immune response can result in a disseminated form of zoster that includes severe multi-organ disease.[2, 9] There is an increased risk of airborne transmission of VZV for immunocompromised individuals with viraemia.
Other factors associated with an increased risk of developing zoster include splenectomy, chronic pancreatitis, chronic kidney disease, chronic inflammatory skin disease,[10] anxiety and depression,[11, 12] sleep disorders[13] and type 1 and type 2 diabetes,[14, 15, 16] chronic obstructive pulmonary disease and adult asthma.[17] Environmental factors such as exposure to high ambient temperature, UV radiation[18, 19] and high altitudes[20] have also been proposed as potential triggers. There is some evidence that a family (sibling or parent) history of zoster is also a potential risk factor in elderly individuals[21] Incidence of zoster is higher in women than men.[4]
25.3. Epidemiology
25.3.1. Global burden of disease
25.3.1. Global burden of disease
Zoster is a sporadic disease occurring as a reactivation of the VZV in individuals who have previously had chickenpox. Approximately one in three people will develop zoster during their lifetime with the incidence rising as cell-mediated immunity to VZV declines with age;[22] 50 percent of those aged 85 years or over will suffer zoster.[23, 24] A systematic review documented an incidence rate between 3 and 5 per 1,000 person-years in North America, Europe and Asia-Pacific.[3] The incidence rate was about 6–8 per 1,000 person-years at age 60 years and 8–12 per 1,000 person-years at age 80 years.
Recurrence is greater in females than males (about 7 percent after eight years compared with 4 percent for males), and in those who are immunocompromised. Third episodes are rare. In those who have zoster at a younger age (45–54 years) the time from the first episode to recurrence is shorter than for those who are aged over 55 years (mean time 2 years [IQR 1.0–2.3] vs 3 years [1.4–4.2], respectively).[25]
VZV is present in lesions of zoster and is transmissible via direct contact with the vesicles to other susceptible individuals (causing chickenpox). Airborne transmission can occur from immunocompromised individuals with disseminated zoster. Episodes of zoster in older individuals provide a constant mechanism for reintroducing the virus, causing varicella in non-immune individuals who are in close contact, who then spread the virus to other susceptible individuals.
Following the introduction of VV onto the childhood schedule, exposure to wild-type virus decreases. It has been theorised that a lack of boosting may lead to an increase in zoster in older adults. However, several studies that have investigated this issue, observed an increase in zoster prior to VV programme introductions and have been unable to attribute any increase in incidence of zoster to childhood VV programmes.[11, 12, 13, 14] Such increases have been observed in countries both with and without childhood varicella immunisation.
25.3.2. New Zealand epidemiology
25.3.2. New Zealand epidemiology
Zoster hospitalisations by age group during 2018/2019 are shown in Figure 25.1, with around 60 percent occurring in adults aged 60 years and older. Hospitalisations are predicted to account for only a very small proportion of the overall zoster cases as most are managed in primary care. Interrogation of general practice electronic records found the incidence of zoster in New Zealand to be similar (approximately 5 per 100,000 patient-years rising to 12.8 per 100,000 in those aged 80–90 years) to the global incidence estimates described in section 25.3.1.[26] In 2018/2019, there were 483 hospitalisations associated with herpes zoster.
Figure 25.1: Hospitalisations with herpes zoster as primary diagnosis by age group, 2018/2019
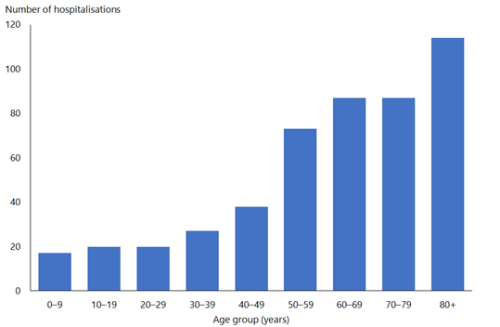
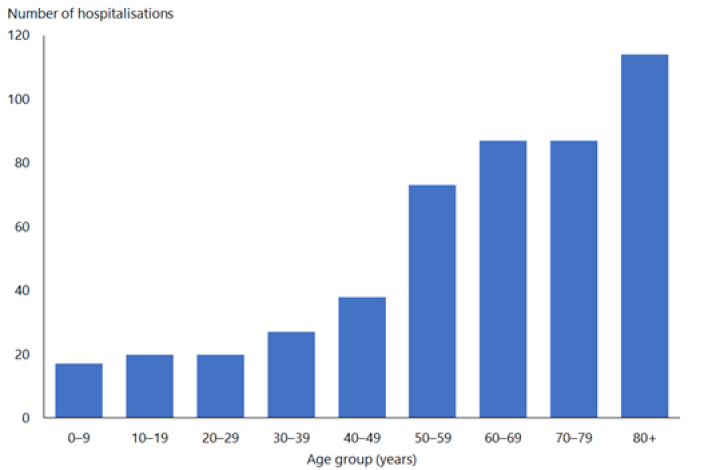
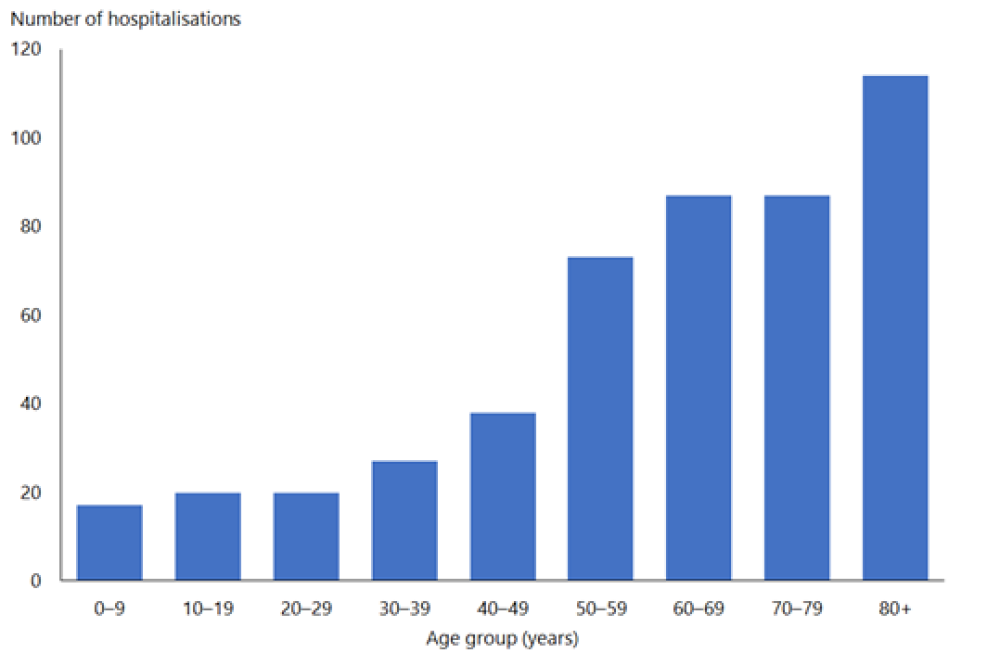
| Source: Ministry of Health. |
25.4. Vaccine
25.4.1. Available vaccines
25.4.1. Available vaccines
Funded vaccine
The funded vaccine is an adjuvanted recombinant subunit zoster vaccine (Shingrix, GSK) containing recombinant VZV glycoprotein E and a proprietary AS01B adjuvant system that is designed to specifically boost T-cell immunity against VZV.[27]
Each 0.5 ml dose contains:
- 50 µg of recombinant VZV glycoprotein E
- AS01B liposome-based adjuvant containing two immunostimulants: 50 µg of Quillaja saponaria (soapbark tree) saponin fraction 21 (QS-21) with 50 µg detoxified lipopolysaccharide fraction, 3-O-desacyl-4’-monophosphoryl lipid A (MPL), from Salmonella minnesota.
- It also contains dioleoylphosphatidylcholine, cholesterol, sodium chloride, dibasic sodium phosphate, monobasic potassium phosphate and water.
Historical vaccines
A live attenuated varicella-zoster virus vaccine (Zostavax, MSD) is approved for use from the age of 50 years and used as part of the Schedule at age 65 years from 2018 to August 2022. It is no longer available in New Zealand.
25.4.2. Efficacy and effectiveness
25.4.2. Efficacy and effectiveness
Efficacy in adults aged 50 years and over
Two phase III clinical trials (ZOE-50 and ZOE-70) demonstrated vaccine efficacy of over 90 percent in adults aged from 50 years and aged over 70 years, and those with medical conditions that increase their risk of zoster.[28, 29, 30, 31, 32] Pooled data gave vaccine efficacy of 91 percent (95% CI 87–95 percent) against the incidence of zoster overall, and 91 percent (86–98 percent) against post-herpetic neuralgia across all age groups. No decline in efficacy was observed with increasing age; in those aged over 80 years efficacy was 91 percent (80–97 percent) against zoster.[33]
Immunogenicity of rZV was shown to be similar in adults aged 65 or over who have previously received live zoster vaccine compared with those who were live ZV naïve. A strong humoral and polyfunctional cell-mediated immune response was shown to persist for at least 1 year after dose 2 of rZV.[34]
Post-hoc analysis, long term follow-up of trial participants found rZV efficacy against zoster plateaued after four to six years and was sustained overall at 84 percent for at least seven years and 70 percent at up to ten years post-vaccination, including in individuals aged 70 years and over and people with pre-existing medical conditions.[29, 33, 35]
Effectiveness in adults aged 50 years and over
Many of the effectiveness studies of recombinant ZV have been conducted in the US.. A systematic review reported that observational studies have confirmed the high effectiveness of two doses of rZV against zoster (ranging from 70 to 85 percent). [36]
One observational study involving 1.74 million people found the vaccine effectiveness of two doses of rZV against zoster overall was 85.5 percent (95% CI 83.5–87.3 percent), 86.8 percent (84.6–88.7 percent) in those aged 50 to 79 years and 80.3% (75.4–84.3 percent) for those aged 80 years and over. In those who had received live ZV within the previous 5 years, vaccine effectiveness of recombinant ZV was 84.8 percent (75.3–90.7 percent) compared with unvaccinated people. Adjusted effectiveness of two doses rZV against herpes zoster ophthalmicus was 89.1 percent (82.9–93.0 percent).[37]
Another real-world study of Medicare beneficiaries in the US found that administering the second dose beyond six months after the first dose did not impair effectiveness in community-dwelling adults aged over 65 years (approximately 1.5 million participants received one dose and 1.0 million received two doses, compared with 15.6 million unvaccinated controls).[38] One dose was 59.5 percent (57.4–61.4 percent) effective for up to six months and 43.5 percent (37.9–48.7 percent) after six months; whereas, two doses were 70.0 percent (68.4–71.5 percent) effective for up to six months after the second dose, and effectiveness was maintained beyond six months. [38] This study showed that vaccine effectiveness of two doses was lower for those with immunosuppressive conditions (64.1 percent; 95% CI 57.2-69.8) and those with autoimmune disease (68.0 percent; 95% CI 62.3-72.8) than immunocompetent individuals (70.5 percent; 95% CI 69.0-72.0). [38]
Severely immunocompromised adults
Good immunogenicity was also shown in younger immunocompromised participants, including those aged from 18 years with solid organ transplants, solid organ tumours, haematopoietic stem cell transplants or living with HIV infection.[39, 40, 41, 42, 43] In HSCT recipients, efficacy of 72 percent (39–88%) was shown in those aged 18–49 years and 67 percent (53–78 percent) in those aged 50 or older with 21 months follow-up; in those aged from 18 years with haematological malignancies, efficacy was estimated at 87.2 percent (44.3–98.6 percent) for up to 13 months post vaccination.[40] To date, there is limited data in real-world settings or long term follow-up for those aged 18-49 years with severe immunocompromise.
25.4.3. Transport, storage and handling
25.4.3. Transport, storage and handling
Transport according to the National Standards for Vaccine Storage and Transportation for Immunisation Providers 2017 (2nd edition).
The recombinant rZV (Shingrix) must be reconstituted before use with supplied diluent. Once reconstituted, if not used promptly, can be store in a refrigerator (+2°C to +8°C) for up to 6 hours. Do not freeze. Protect from light.
25.4.4. Dosage and administration
25.4.4. Dosage and administration
Two doses of 0.5 ml are administered intramuscularly from two to six months apart.
If a shortened schedule is required, the second dose can be given optimally at two months after the first dose.
Serological testing for previous VZV infection is not necessary prior to administration of this rZV to individuals with immunocompromise.
Individuals who are receiving antiviral medications, such as acyclovir, can be given rZV at any time without discontinuing their treatment. This vaccine does not contain live varicella-zoster virus.
Co-administration with other vaccines
Recombinant ZV can be co-administered with all the vaccines available on the Schedule, including seasonal influenza vaccine, mRNA-CV, 23PPV and Tdap. It can also be given at any time with the adjuvanted influenza vaccine aQIV (FluAd Quad) or RSVPreF, preferably in a different limb. When RSVPReF and rZV are given together, mild to moderate reactions, such as injection-site pain and fatigue, can occur more frequently than when given separately due to receiving additional AS01 adjuvant.
25.5. Recommended immunisation schedule
Table 25.1: Herpes zoster vaccine (rZV) recommendations
Table 25.1: Herpes zoster vaccine (rZV) recommendations
| Note: Neither history of previous varicella infection nor evidence of prior immunity to VZV is required prior to the routine administration of rZV. Funded individuals are shown in the shaded row. See the Pharmaceutical Schedule for any changes to funding decisions. |
|
Recommended and funded |
|---|
|
Two doses of recombinant rZV are funded:
|
|
For consideration, but not funded |
|
Two doses of recombinant rZV are recommended but not funded for all individuals aged from 50 years, including those aged over 66 years; and for individuals aged from 18 years who are at increased risk of zoster [5, 6, 44, 45, 46] including:
Other conditions that can increase risk of zoster in older adults include: [10, 12, 14,]
|
|
a. The second dose is funded at age 66 years if the first dose was given at age 65 years. b. Including those with a past-history of haematological malignancy who remain immunocompromised c. People living with advanced or untreated HIV infection with CD4 counts <350/µL or those with a higher CD4 count not established on effective anti-retroviral therapy (i.e. with a viral load of >500 copies / mL or 2.7 Log10) d. Ideally, vaccinate prior to planned immunosuppression. If rZV is given during treatment regimen, take timing of treatment and level of immunosuppression into consideration when timing vaccinations. If a shortened schedule is required, the second doses can be given optimally at two months after the first dose. |
25.5.1. Recommended and funded
25.5.1. Recommended and funded
Two doses of adjuvanted recombinant zoster vaccine (rZV; Shingrix) are recommended and funded for all adults at the age of 65 years. The second dose continues to be funded for those who turn age 66 years between doses, but not beyond the age of 66 (ie age 67 years and over), unless eligible as below.
RZV is also available for individuals aged 18 years and older at increased risk of zoster, particularly those who are at increased risk of zoster due to comorbidities.[4, 7, 44] Two doses of rZV are funded for individuals aged 18 years and over, including those aged 66 years and over, who are pre and post haematopoietic stem cell transplantation or cellular therapy; due to receive or following solid organ transplant; with haematological malignancies; living with poorly controlled HIV infection; with certain immune-mediated inflammatory disease (autoimmune diseases) receiving disease-modifying immunomodulatory agents (formerly known as DMARDS, biologic, synthetic or conventional); with end-stage chronic kidney disease (CKD-4 or -5); or primary immunodeficiencies (see Table 24.1 for funded groups).
It is recommended to discuss the optimal timing for vaccination with a specialist before the vaccine appointments for those who are severely immunocompromised. Ideally, vaccination should be conducted prior to any planned immunosuppression (see section 4.3.6). If a shortened schedule is required, the second doses can be given optimally at two months after the first dose.
25.5.2. Recommended not funded
25.5.2. Recommended not funded
rZV is approved for use in New Zealand for all individuals aged 50 years or older, including those aged 66 years and over, not eligible to funded vaccine.
It is also available (unfunded) for individuals aged 18 years and older at increased risk of zoster. This particularly includes those with comorbidities,[4, 7, 44] and includes individuals aged 66 years and over who did not receive rZV at age 65 years. These groups include individuals who are immunocompromised due to an existing illness and/or its treatment or prior to planned immunosuppression; those receiving immunomodulatory therapy; or chemotherapy or systemic radiotherapy; or living with well-controlled HIV infection (see Table 24.1 for recommended but not funded groups).
It is recommended to discuss the optimal timing for vaccination with a specialist before the vaccine appointments for those who are severely immunocompromised. Ideally, vaccination should be conducted prior to any planned immunosuppression (see section 4.3.6). If a shortened schedule is required, the second doses can be given optimally at two months after the first dose.
25.5.3. Individuals with a history of zoster (shingles)
25.5.3. Individuals with a history of zoster (shingles)
Individuals with a history of zoster episodes can be given rZV. It is possible that a history of previous zoster may be inaccurate or a mistaken diagnosis. [44] In addition, the risk of a repeat episode of zoster has been estimated at approximately 5 percent in immunocompetent individuals. [25, 44] The incidence of recurrence is higher in women than men, in people who are immunosuppressed, and in those aged 45–64 years compared with those aged over 65 years at the time of the first episode. [25]
There are no recognised safety concerns in giving zoster vaccines to people with a history of zoster episodes. [47, 48] The length of time following an episode of zoster after which it may be beneficial to vaccinate has not been established. [49] Recombinant ZV is recommended to be given from 12 months after zoster has resolved from which time the rate of recurrence is increased. [25, 49] Caution is required for individuals who have previously experienced ocular complications of zoster, such as herpes zoster ophthalmicus and uveitis, in this case vaccination is not recommended until at least 12 months after the inflammation has completely resolved.
25.5.4. Individuals with a history of zoster vaccination
25.5.4. Individuals with a history of zoster vaccination
The optimal time for administration of recombinant zoster vaccine following live zoster vaccination (Zostavax) is not yet established. [49] Effectiveness of live zoster vaccine wanes significantly within three to five years of vaccination in adults aged 60 or older. [34] Individuals who previously received live zoster vaccine can receive two doses of recombinant ZV (see Table 24.1 for funded and recommended groups). Spacing of at least 12 months after live zoster vaccine is recommended but timing may be shortened to three months for the use of rZV in individuals who are immunocompromised with an increased risk of zoster recurrence or prior to planned immunosuppression.
25.6. Contraindications and precautions
See section 2.1.3 for pre-vaccination screening guidelines and section 2.1.4 for general contraindications for all vaccines.
25.6.1. Contraindications
25.6.1. Contraindications
Recombinant rZV (Shingrix) is contraindicated to individuals with a history of hypersensitivity to a previous dose or to any component of the vaccine.
25.6.2. Precautions
25.6.2. Precautions
There is limited data on the use of rZV in human pregnancy however, since it is a non-live vaccine, there are no theoretical safety concerns should it be inadvertently administered during pregnancy.
25.7. Potential responses and AEFIs
25.7.1. Potential responses
25.7.1. Potential responses
During clinical trials, rZV was generally well tolerated. The most commonly reported responses were injection-site pain, myalgia and fatigue; other responses included headache, shivering, fever and gastrointestinal symptoms. These were mild to moderate and lasting for one to three days post vaccination, with higher incidence in those aged under 70 years than in the older age groups.[31] Adverse events were also more frequently reported in younger age groups (ages 18 to 49 years compared with those aged over 50 years). In clinical studies in those aged 50 years and over, a higher incidence of fever and shivering was reported when rZV was co-administered with 23PPV.[50]
Fever and shivering are reported more frequently when rZV is coadministered with 23PPV than when rZV is given alone.
25.7.2. AEFIs
25.7.2. AEFIs
Injection-site reactions (eg redness or swelling) were more common after vaccination with rZV than live ZV according to a meta-analysis of clinical trial data (risk difference of 30 percent; 95% CI 2 to 51 percent). There was no statistical difference between serious adverse events or study withdrawal due to adverse events.[51] No safety concerns in immunocompromised populations were associated with rZV across six clinical trials; most adverse events reported were consistent with the underlying diseases or treatments and similar between vaccinated and placebo controls.[52] A post-market surveillance study in adults aged 65 years or over observed a slightly increased risk of Guillain-Barré syndrome (estimated three excess cases per million doses) during 42 days following vaccination with rZV.[50]
There have been rare reports of flares of pre-existing inflammatory eye disease including uveitis and herpes zoster ophthalmicus following rZV administration.[53, 54] It is recommended to allow at least 12 months after ocular zoster episode had resolved prior to administering rZV.
In a small clinical trial (865 adults aged 50 years and over), fever and shivering were reported more frequently when PPV23 was co-administered with rZV than when rZV was given alone (16 percent and 21 percent versus 7 percent each).[50]
25.8. Variations from the vaccine data sheet
None.
References
References
References
- Gilden D. Efficacy of live zoster vaccine in preventing zoster and postherpetic neuralgia. J Intern Med, 2011. 269(5): p. 496-506.
- Gershon A, Marin M ,Seward JF. 2018. Varicella vaccines, in Plotkin's Vaccines (7th edition), Plotkin S, Orenstein W, Offit P, and Edwards K (eds). Elsevier: Philadelphia, US.
- Kawai K, Gebremeskel BG ,Acosta CJ. Systematic review of incidence and complications of herpes zoster: towards a global perspective. BMJ Open, 2014. 4(6): p. e004833.
- Kawai K ,Yawn BP. Risk factors for herpes zoster: a systematic review and meta-analysis. Mayo Clin Proc, 2017. 92(12): p. 1806-1821.
- Muñoz-Quiles C, López-Lacort M, Díez-Domingo J,Orrico-Sánchez A. Herpes zoster risk and burden of disease in immunocompromised populations: a population-based study using health system integrated databases, 2009-2014. BMC Infect Dis, 2020. 20(1): p. 905.
- Kho MML, Roest S, Bovée DM, et al. Herpes zoster in solid organ transplantation: incidence and risk factors. Front Immunol, 2021. 12: p. 645718.
- Yenikomshian MA, Guignard AP, Haguinet F, et al. The epidemiology of herpes zoster and its complications in Medicare cancer patients. BMC Infect Dis, 2015. 15: p. 106.
- Che H, Lukas C, Morel J,Combe B. Risk of herpes/herpes zoster during anti-tumor necrosis factor therapy in patients with rheumatoid arthritis. Systematic review and meta-analysis. Joint Bone Spine, 2014. 81(3): p. 215-21.
- Gnann JW, Jr. ,Whitley RJ. Clinical practice. Herpes zoster. N Engl J Med, 2002. 347(5): p. 340-6.
- Chovatiya R ,Silverberg JI. Association of herpes zoster and chronic inflammatory skin disease in US inpatients. J Am Acad Dermatol, 2021. 85(6): p. 1437-1445.
- Liao CH, Chang CS, Muo CH,Kao CH. High prevalence of herpes zoster in patients with depression. J Clin Psychiatry, 2015. 76(9): p. e1099-104.
- Choi HG, Kim EJ, Lee YK,Kim M. The risk of herpes zoster virus infection in patients with depression: A longitudinal follow-up study using a national sample cohort. Medicine (Baltimore), 2019. 98(40): p. e17430.
- Chung WS, Lin HH ,Cheng NC. The incidence and risk of herpes zoster in patients with sleep disorders: a population-based cohort study. Medicine (Baltimore), 2016. 95(11): p. e2195.
- Huang CT, Lee CY, Sung HY, et al. Association between diabetes mellitus and the risk of herpes zoster: A systematic review and meta-analysis. J Clin Endocrinol Metab, 2022. 107(2): p. 586-597.
- Lai SW, Liu CS, Kuo YH, et al. The incidence of herpes zoster in patients with diabetes mellitus: A meta-analysis of cohort studies. Medicine (Baltimore), 2021. 100(16): p. e25292.
- Guignard AP, Greenberg M, Lu C, et al. Risk of herpes zoster among diabetics: a matched cohort study in a US insurance claim database before introduction of vaccination, 1997-2006. Infection, 2014. 42(4): p. 729-35.
- Peng YH, Fang HY, Wu BR, et al. Adult asthma is associated with an increased risk of herpes zoster: A population-based cohort study. Journal of Asthma, 2017. 54(3): p. 250-257.
- Kawai K, VoPham T, Drucker A, et al. Ultraviolet radiation exposure and the risk of herpes zoster in three prospective cohort studies. Mayo Clin Proc, 2020. 95(2): p. 283-292.
- Lai SW, Liao KF, Kuo YH, et al. The impacts of ambient temperature and ultraviolet radiation on the incidence of herpes zoster: An ecological study in Taiwan. Int J Clin Pract, 2021. 75(4): p. e13854.
- Singh GK, Deora MS, Grewal R, et al. Is high altitude a risk factor in development of herpes zoster? High Alt Med Biol, 2018. 19(3): p. 244-248.
- Tseng HF, Chi M, Hung P, et al. Family history of zoster and risk of developing herpes zoster. International Journal of Infectious Diseases, 2018. 66: p. 99-106.
- Wehrhahn M ,Dwyer D. Herpes zoster: epidemiology, clinical features, treatment and prevention. Australian Prescriber, 2012. 35(5): p. 143–7.
- Brisson M, Edmunds WJ, Law B, et al. Epidemiology of varicella zoster virus infection in Canada and the United Kingdom. Epidemiol Infect, 2001. 127(2): p. 305-14.
- Schmader K. Herpes zoster in older adults. Clin Infect Dis, 2001. 32(10): p. 1481-6.
- Qian J, Macartney K, Heywood AE, et al. Risk of recurrent herpes zoster in a population-based cohort study of older adults. J Am Acad Dermatol, 2021. 85(3): p. 611-618.
- Turner NM, MacRae J, Nowlan ML, et al. Quantifying the incidence and burden of herpes zoster in New Zealand general practice: a retrospective cohort study using a natural language processing software inference algorithm. BMJ Open, 2018. 8(5): p. e021241.
- Heineman TC, Cunningham A ,Levin M. Understanding the immunology of Shingrix, a recombinant glycoprotein E adjuvanted herpes zoster vaccine. Curr Opin Immunol, 2019. 59: p. 42-48.
- Cunningham AL, Lal H, Kovac M, et al. Efficacy of the herpes zoster subunit vaccine in adults 70 years of age or older. N Engl J Med, 2016. 375(11): p. 1019-32.
- Dagnew AF, Rausch D, Hervé C, et al. Efficacy and serious adverse events profile of the adjuvanted recombinant zoster vaccine in adults with pre-existing potential immune-mediated diseases: a pooled post hoc analysis on two parallel randomized trials. Rheumatology (Oxford), 2021. 60(3): p. 1226-1233.
- Oostvogels L, Heineman TC, Johnson RW, et al. Medical conditions at enrollment do not impact efficacy and safety of the adjuvanted recombinant zoster vaccine: a pooled post-hoc analysis of two parallel randomized trials. Hum Vaccin Immunother, 2019. 15(12): p. 2865-2872.
- Syed YY. Recombinant zoster vaccine (Shingrix®): a review in herpes zoster. Drugs Aging, 2018. 35(12): p. 1031-1040.
- Lal H, Cunningham AL, Godeaux O, et al. Efficacy of an adjuvanted herpes zoster subunit vaccine in older adults. N Engl J Med, 2015. 372(22): p. 2087-96.
- Boutry C, Hastie A, Diez-Domingo J, et al. The adjuvanted recombinant zoster vaccine confers long-term protection against herpes zoster: Interim results of an extension study of the pivotal phase III clinical trials (ZOE-50 and ZOE-70). Clin Infect Dis, 2022. 74(8): p. 1459-1467.
- Dagnew AF, Klein NP, Hervé C, et al. The Adjuvanted Recombinant Zoster Vaccine in Adults Aged ≥65 Years Previously Vaccinated With a Live-Attenuated Herpes Zoster Vaccine. J Infect Dis, 2021. 224(7): p. 1139-1146.
- Strezova A, Diez-Domingo J, Al Shawafi K, et al. Long-term Protection Against Herpes Zoster by the Adjuvanted Recombinant Zoster Vaccine: Interim Efficacy, Immunogenicity, and Safety Results up to 10 Years After Initial Vaccination. Open Forum Infect Dis, 2022. 9(10): p. ofac485.
- Zeevaert R, Thiry N, Maertens de Noordhout C,Roberfroid D. Efficacy and safety of the recombinant zoster vaccine: A systematic review and meta-analysis. Vaccine X, 2023. 15: p. 100397.
- Lu A, Sun Y, Porco TC, et al. Effectiveness of the recombinant zoster vaccine for herpes zoster ophthalmicus in the United States. Ophthalmology, 2021. 128(12): p. 1699-1707.
- Izurieta HS, Wu X, Forshee R, et al. Recombinant zoster vaccine (Shingrix): Real-world effectiveness in the first 2 years post-licensure. Clin Infect Dis, 2021. 73(6): p. 941-948.
- Anderson TC, Masters NB, Guo A, et al. Use of recombinant zoster vaccine in immunocompromised adults aged ≥19 years: Recommendations of the Advisory Committee on Immunization Practices - United States, 2022. MMWR Morb Mortal Wkly Rep, 2022. 71(3): p. 80-84.
- Racine E, Gilca V, Amini R, et al. A systematic literature review of the recombinant subunit herpes zoster vaccine use in immunocompromised 18-49 year old patients. Vaccine, 2020. 38(40): p. 6205-6214.
- Berkowitz EM, Moyle G, Stellbrink HJ, et al. Safety and immunogenicity of an adjuvanted herpes zoster subunit candidate vaccine in HIV-infected adults: a phase 1/2a randomized, placebo-controlled study. J Infect Dis, 2015. 211(8): p. 1279-87.
- Vink P, Delgado Mingorance I, Maximiano Alonso C, et al. Immunogenicity and safety of the adjuvanted recombinant zoster vaccine in patients with solid tumors, vaccinated before or during chemotherapy: A randomized trial. Cancer, 2019. 125(8): p. 1301-1312.
- Vink P, Ramon Torrell JM, Sanchez Fructuoso A, et al. Immunogenicity and safety of the adjuvanted recombinant zoster vaccine in chronically immunosuppressed adults following renal transplant: A phase 3, randomized clinical trial. Clin Infect Dis, 2020. 70(2): p. 181-190.
- Australian Technical Advisory Group on Immunisation (ATAGI). 2022. Zoster (herpes zoster). in Australian Immunisation Handbook. Canberra. URL: https://immunisationhandbook.health.gov.au/vaccine-preventable-diseases/zoster-herpes-zoster. (accessed 2 August 2022)
- Gilbert L, Wang X, Deiss R, et al. Herpes zoster rates continue to decline in people living with human immunodeficiency virus but remain higher than rates reported in the general US population. Clin Infect Dis, 2019. 69(1): p. 155-158.
- Lai SW, Kuo YH, Lin CL,Liao KF. Risk of herpes zoster among patients with predialysis chronic kidney disease in a cohort study in Taiwan. Int J Clin Pract, 2020. 74(10): p. e13566.
- Centers for Disease Control and Prevention. 2018 Zostavax recommendations. 2018; URL: https://www.cdc.gov/vaccines/vpd/shingles/hcp/zostavax/recommendations.html. (accessed 20 May 2020)
- Godeaux O, Kovac M, Shu D, et al. Immunogenicity and safety of an adjuvanted herpes zoster subunit candidate vaccine in adults ≥ 50 years of age with a prior history of herpes zoster: A phase III, non-randomized, open-label clinical trial. Hum Vaccin Immunother, 2017. 13(5): p. 1051-1058.
- ATAGI. 2022 Statement on the clinical use of zoster vaccines in adults in Australia. Australian Government Department of Health. URL: https://www.health.gov.au/resources/publications/statement-on-the-clinical-use-of-zoster-vaccine-in-older-adults-in-australia. (accessed 2 August 2022)
- GlaxoSmithKline NZ Ltd. 2022 New Zealand datasheet: Shingrix. URL: https://www.medsafe.govt.nz/profs/datasheet/s/shingrixinj.pdf. (accessed 3 August 2022)
- Tricco AC, Zarin W, Cardoso R, et al. Efficacy, effectiveness, and safety of herpes zoster vaccines in adults aged 50 and older: systematic review and network meta-analysis. BMJ, 2018. 363: p. k4029.
- López-Fauqued M, Co-van der Mee M, Bastidas A, et al. Safety profile of the adjuvanted recombinant zoster vaccine in immunocompromised populations: An overview of six trials. Drug Saf, 2021. 44(7): p. 811-823.
- Tavares-Da-Silva F, Co MM, Dessart C, et al. Review of the initial post-marketing safety surveillance for the recombinant zoster vaccine. Vaccine, 2020. 38(18): p. 3489-3500.
- Walia A, Sun Y ,Acharya NR. Risk of Herpes Zoster Ophthalmicus Recurrence After Recombinant Zoster Vaccination. JAMA Ophthalmol, 2024. 142(3): p. 249-256.