Appendix 2: Low gestational sac in the first trimester with previous caesarean section
Appendix 2 for the New Zealand Obstetric Ultrasound Guidelines.
The presence of a sac located in an abnormally low position within the uterus in the first trimester in a woman who has had one or more caesarean sections should prompt careful further review, including transvaginal (TV) scanning, if possible.
The differential diagnosis includes a normally developing but low sac that shows normal subsequent development on follow-up scans, an inevitable miscarriage (which appears avascular), scar ectopic or abnormally adherent trophoblast/placenta (early evidence of placenta accreta/abnormally implanted placenta).
The trophoblast is directly implanted over the scar. These cases may be very difficult to differentiate from scar ectopic pregnancies.
A TV ultrasound scan is recommended to assess location of the pregnancy. Implantation into the previous caesarean section scar can be diagnosed when:
The scar may be thin, or deficient, with a visible gap in the myometrium of the anterior uterine wall. The gestational sac may bulge towards the bladder in these cases.
From about 16 weeks, irregular vascular sinuses appear, with turbulent flow.
The bladder wall may appear interrupted or have small bulges of the placenta into the bladder space. Absence of the normal retroplacental ‘clear zone’ (the echolucent space between the placenta and myometrium) may be unreliable.
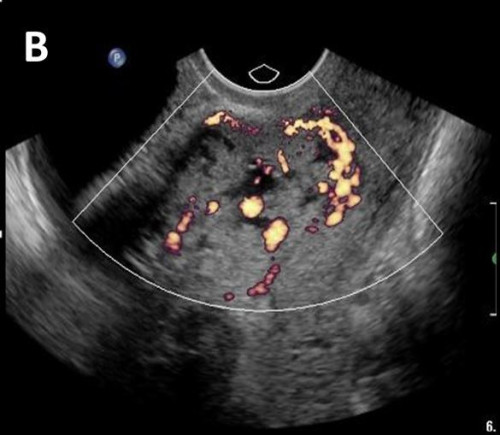
Colour Doppler may show placental bed hypervascularity and that some of the placental sinuses traverse the uterine wall.


Low implantation of the gestational sac in a retroverted uterus (TV scan) (A), with the sac deviated anteriorly into the scar, arrows (B), suspicious for early accreta / abnormal trophoblast implantation.
Scans later in pregnancy showed complete placenta previa and accreta.
The pregnancy is entirely contained within the myometrial confines of the scar, with no part within the cavity itself, unlike in first-trimester cases of abnormally implanted trophoblast/placenta accreta.
Abnormal trophoblastic tissue implanted entirely within the confines of the caesarean section scar, separate from the endometrial cavity (arrows), in greyscale (A), and colour Doppler (B).